We are launching the new Laboratory Information Management System (LIMS) within Pathology on Monday 10 November.
CliniSys Winpath Enterprise will be replacing our current LIMS and is designed to manage laboratory data, samples, and workflows. There are many benefits to upgrading our LIMS including:
- Improved collaboration
- Data integrity and quality control
- Cost efficiency
- Compliance and audit trails
What can GP’s do to help minimise delay- managing advanced orders
To enable us to make a smooth transition over to the new system we kindly ask that:
- Where possible, please minimise the creation of non-urgent biochemistry and haematology ICE requests in the weeks prior to Monday 10 November. This is to ensure there is not a backlog of legacy requests that will need to be entered manually onto the new LIMS when they sample arrives in the lab.
- Alternatively, if it is possible to remake any legacy requests in ICE after Monday 10 November, this would also be extremely helpful.
- All microbiology samples are to be processed as normal.
- Patients are encouraged to come in for their routine biochemistry and haematology blood tests prior to Monday 10 November.
- Where possible, phlebotomy clinics are moved to later during the week and not on Monday 10 November.
As a result of the implementation of the new system, turnaround times for routine results may be delayed, so please be mindful and escalate any urgent requests as normal.
From Monday 10 November, you may notice a difference in the format or order of certain Pathology results. This is due to standardisation between the laboratories that share the LIMS that Portsmouth Hospitals University NHS Trust is moving to and therefore cannot be changed. Please see the FAQs for an example.
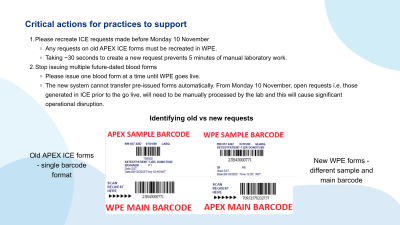
Cease issuing blood test request forms
To ensure a smooth transition and to mitigate significant operational challenges, we kindly request that GPs immediately cease issuing blood test request forms that are intended to be used in the future i.e. “legacy forms” via ICE. Please limit the distribution to one blood test form at a time until the new system is fully implemented.
This request is critical because the new LIMS will not support the automatic transfer of pre-issued blood forms. Failure to comply with this will result in significant operational disruption in the laboratory. We are actively working to avoid the scenario experienced at another Trust, where, following transition to the new system, the absence of this precaution led to manually re-entering thousands of outstanding blood test requests during their go-live week, which impacted the laboratory’s capacity and caused delays to patient care.
We ask for your cooperation to prevent this workload and disruption at Portsmouth Hospitals. Your support in adhering to this temporary measure will be invaluable to ensuring a successful system go-live and continued high-quality pathology services.
AKI reporting immediately post LIMS go live
From midnight on Sunday 9 November until Thursday 20 November, we will be unable to calculate AKI accurately for any patient where the previous creatinine results over the last year fall between 15 September and midnight 9 November. This is due to a temporary unavoidable gap in creatinine data migration from the old LIMS.
You will need to check in your usual downstream system (Minestrone/ICE/GP IT system) to see whether the patient has a previous creatinine result between 15 September and midnight 19 November inclusive and then assess the AKI risk as follows:
Divide the current creatinine result by the previous creatinine result (or the lowest previous creatinine result if there is more than one) to calculate the relative difference.
| Relative difference | AKI score |
|---|---|
| <1.5 | No AKI alert |
| 1.5-1.9 | AKI 1 |
| 2.0-2.9 | AKI 2 |
| >2.9 | AKI 3 |
This is a stop gap for 10 days after go live until the data migration is complete. Normal AKI reporting will resume after this time.
As an additional risk mitigation, there will be a temporary process for phoning creatinine results. When the creatinine result is elevated and there is no previous creatinine in the past year, the creatinine result is reported with a comment “Elevated creatinine - ?AKI, ?CKD – suggest repeat”. From midnight on Sunday 9 November until Thursday 20 November, all results generating this comment will be phoned to the requesting source.
| Question | Answer |
|---|---|
| What is the PHU LIMS? | Portsmouth Hospital University NHS Trust (PHU) Laboratory Information Management System (LIMS) underpins Pathology test requests and results. At the GP practice, you will not directly interact with the LIMS but it is integral to the end to end system and connects to ICE. |
| When is the new PHU LIMS go live? | Monday 10 November |
| Are any IT configuration changes required to my GP practice computer system? | Yes, you need to register a new EDI trader code to ICE. |
| Have I been told about this new EDI trader code? | Yes, the PHU project team has been communicating this since 2023. Please check your emails for communications from sender pho-tr. |
| What do I do if I have not heard from the PHU project team about EDI trader codes? | Please get in touch by contacting pho-tr. |
| What is the new EDI trader code I require? | The new trader code is 110000042100008 |
| How do I register the EDI trader code for my TPP SystmOne system? |
SystmOne practices will need to ask TPP to add the trader code before they can register. |
| How do I register the EDI trader code for my EMIS system? | EMIS sites should be able to add the code and register directly. |
| What happens if I am unable to register the EDI trader code in EMIS myself? | Contact your EMIS helpdesk for guidance. |
| What happens if I have not registered the EDI trader code? | You will be unable to submit requests or receive results from the new LIMS from the go-live date. |
|
Will there be any noticeable differences after Monday 10 November? |
You will still access your GP practice system the same way and submit requests as usual. When requesting bloods, you'll be redirected to the WPE (WinPath) panels instead of the APEX panels (the tests within the panels will be the same, they are just aimed at the new LIMS instead of the old one). We have outlined some differences that will take affect from Monday 10 November: 1. Microbiology unit change - All Microbiology Urine samples processed for microscopy and culture will have a different unit of measurement. These results will be reported as per Litre and therefore will have a higher exponentiation figure than currently seen. 2. Reference range changes - There will be a change in reference ranges for some tests, to support standardisation across the wider network. For example, FBC (Full Blood Count). Please follow this link to view detail of the range changes. 3. Antibiotics reporting - The way antibiotics are input to the new LIMS has changed, meaning the presentation of antibiotic information in reports will be different compared to how it was previously displayed. 4. Consolidation of read codes - Some tests that previously had multiple read codes will now be merged into a single code. For example, Urine Microscopy, which was previously represented by separate codes for different components, will now be recorded under a single read code. 5. Text display order - There will be minor differences in how results are displayed, specifically, some tests that contain multiple results within the same category (i.e. Full Blood Count - FBC) may have their display order altered, for e.g. in WPE, the White Blood Count (WBC) appears above Haemoglobin (Hb), whereas in APEX the order is reversed. This change is inherent to how WPE displays the FBC and unfortunately cannot be adjusted. 6. New categorisation for some tests - There are tests that previously appeared under multiple read codes that will now be grouped under one. For example, TB cultures, which were previously listed under "Mycobacteria MC&S" will now be categorised under Sample Culture. In WPE, tests are booked under Sample Culture, with the specific sample type (e.g. urine, blood, sputum) selected afterward. 7. Report printing format - When printing, you'll notice that many tests now have their own dedicated column, ensuring that results are clearly organised. 8. Formatting of test description - Test descriptions now appear in capital letters. This is part of the standard format and cannot be adjusted locally. 9. Report transmission timing - On the current system, pathology reports are typically transmitted overnight. With the new LIMS, reports will be transmitted in real time, as they're issued. This means results may appear in your system throughout the day, rather than in a single batch. Changes to result reporting:
|
| Will there be any service disruption to requests from the go-live date? |
No, you will be able to request as normal. However, please note, it is likely that processing of requests will be slower than usual whilst the new system beds in. |
| Will there be any impact to the turnaround time of results? | Yes. For three to four weeks post go-live, issuing of Pathology results from PHU may be slower. This is due to the bedding in of the new system. |
| Has any testing been completed with my GP practice to ensure the LIMS change at PHU will have no negative impact? |
Both TPP SystmOne and EMIS practices will have been tested prior to go live (currently in progress). Two pilot sites, one EMIS and one SystmOne, received comprehensive testing and the remaining practices are being tested with unsolicited results. Extensive testing and validation have been carried out ahead of go-live. While we prioritised the most requested tests based on usage data, we have also validated a wide range of additional tests to ensure clinical safety and continuity. This approach builds on successful implementations at other NHS Trusts and supports a smooth transition to the new LIMS. We are confident that the remaining tests visible on the ICE GP panel page will work as expected, as they follow the same mapping and reporting structure that has already been validated. However, should any individual test be missing a read code at go-live, please be assured of the following:
|
| If I experience any NEW issues with Pathology requesting and resulting after go-live which appear to be linked to the change, what do I do? | If you find any issues that may be related to the change of LIMS, please complete this Incident Form. The form will open on Sunday 9 November and will close on Friday 14 November. Following this date, please refer to your usual BAU processes. |
| For Pathology requests made in ICE before the LIMS go-live, will they still be processed? | Yes, but these will take longer to process because they cannot be automatically transferred onto the LIMS. At time of cutover from old LIMS to new LIMS, all requests made in ICE will be out of date (we call these legacy requests). When the sample arrives at the PHU lab, it will need to be relabelled and manually entered into the LIMS, which is a lot slower. During this time there will be many legacy requests and Lab staff will also be acclimatising to the new LIMS, so there will be delays. Requests that are made in ICE after Monday 10 November, will not be out of date and can be automatically entered onto the LIMS in the usual way. |
| Can we (our practice) do anything to help minimise additional work to us as a result of this change and improve the benefit to patients during and after the go-live? |
Yes:
|
| On and after the go-live, will we be able to access the old system so that we can see the test requests we have in there? | For the avoidance of doubt, you will not be provided with a new version of ICE. You will still be able to see all legacy blood requests and reports through your existing ICE interface. |
| Will we need new blood paper to print onto or does everything line up with what we currently use? | Paper forms will remain the same, with the only change being the barcode. There is no requirement for new forms. |
| EGFR is not present in the U&E results. Why is this? | A U&E panel was not requested. It is likely that individual tests were ordered. Since EGFR is a calculated value based on a full U&E requests, it would not be generated. |
| Why are some Read codes different from what we normally use? | In the new system, tests are requested differently, which means you may see some variations in the Read codes used. This change is expected and is part of how the new system processes requests. It should not impact your local system, but you may notice a difference compared to previous Read codes. |
| Why are some test results missing a Read code? | This is a known behaviour and is already happening with the current system. In the new system, some test results may continue to come through without an assigned Read code. If you require a Read code for a specific result, it will need to be added manually within your own system. |
| What support will be available during the go-live period? |
Several support options will be available during the week of go-live. Full details and access information for the below channels will be shared with practices closer to the launch date:
|